Breast cancer has long been recognised as the most frequently diagnosed cancer among females.1 In 2023 alone, an estimated 2.30 million new cases and over 764,000 deaths were recorded worldwide, marking breast cancer as the leading cause of cancer-related DALYs among women.1,2 Despite improvements in high-income countries, global progress remains uneven.4,5
The Global Burden of Disease 2023 Study provides the most comprehensive epidemiological assessment to date, analysing incidence, mortality, and risk factors across 204 countries over a 34-year period and projecting future trends up to 2050. These findings reveal profound inequities in outcomes, shaped by socioeconomic development, health system capacity, risk factor exposure, and demographic change.2
Rising Incidence Worldwide
Between 1990 and 2023, the global age-standardised incidence rate (ASIR) increased by approximately 16%. In 2023, the ASIR reached 49.3 cases per 100,000 females. However, the global picture conceals deep disparities:2,4
•High-income countries had the highest ASIR (75.7 per 100,000), largely reflecting widespread screening and early detection.
•Low-income and lower-middle-income countries (LICs and LMICs) experienced the largest proportional increases in ASIR—147% and 128% respectively—driven by health system deficits, changing reproductive patterns, and rising obesity.
Divergent Mortality Patterns
While incidence has risen across most of the world, mortality trends diverge sharply:2
•High-income countries saw a 30% reduction in age-standardised mortality rates (ASMR) since 1990 due to improvements in screening, diagnosis, and therapy.
•Low-income countries, by contrast, experienced a near doubling of mortality, with ASMR reaching 24.1 per 100,000—the largest change among all income groups.
Key drivers for these differences include delayed diagnosis, limited access to treatment, inadequate pathology and radiotherapy services, and affordability barriers.2
Disability-Adjusted Life Years (DALYs)
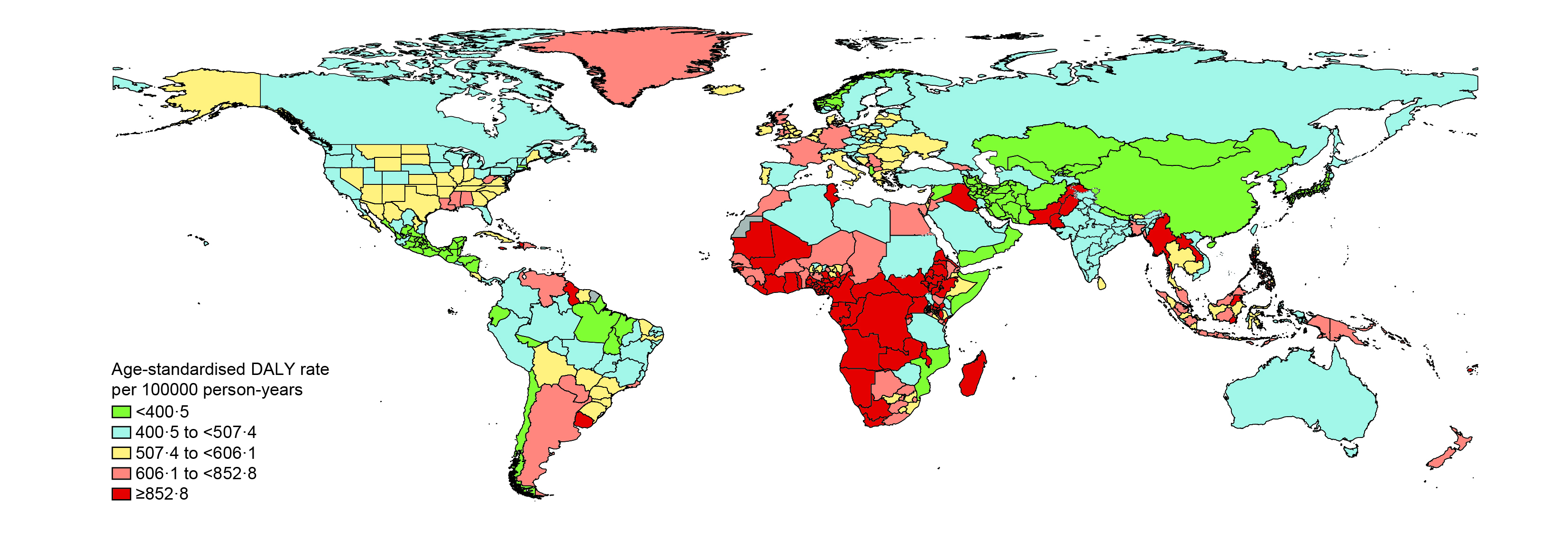
In 2023, breast cancer resulted in 24.1 million DALYs, with more than 90% attributable to premature death (measured as years of life lost [YLLs]). Although high-income countries still account for the largest share of incident cases, nearly half of global DALYs occurred in low- and lower-middle-income settings, illustrating the disproportionate impact of late-stage diagnosis and insufficient treatment capacity (Figure 1).2
High-Income Regions: Progress with Remaining Gaps
High-income countries demonstrate sustained reductions in ASMR and DALYs.2 Five-year survival rates in many of these regions exceed 85–90%.6 Nevertheless, disparities persist within countries:7,8,9
•In the US, mortality among Black women remains 1.4 times higher than among White women.
•Indigenous women in Australia and Māori and Pacific women in New Zealand experience significantly poorer survival.
These differences highlight the importance of addressing structural and social determinants of health even in settings with advanced cancer care infrastructure.
Sub-Saharan Africa: Rapidly Growing Burden
Sub-Saharan Africa recorded the highest mortality rates globally.2 Health system constraints and sociocultural and financial barriers impede timely access to life-saving screenings and diagnosis.10,11,12 In some African countries, fewer than 30% of cases are detected at early stages,4 and survival at three years can be as low as 50%.13
Middle-Income Countries: Expanding Burden Amid Transition
Upper- and lower-middle-income countries (e.g., India, Brazil, Iran) have witnessed sharp increases in incidence. While some progress has been made in building screening and treatment capacity, gaps persist between urban and rural areas, and between insured and uninsured populations. Economic burden has also surged, with countries such as India projecting a near-doubling of breast cancer–related costs by 2030.14,15,16
Lifestyle and Metabolic Risks
The GBD 2023 study identified six key risk factors contributing to breast cancer DALYs:2
•Dietary risks (specifically a diet high in red meat)
•Tobacco use (smoking and second-hand smoke)
•High fasting plasma glucose
•High body mass index (BMI) in adults
•High alcohol consumption
•Low physical activity
In total, these accounted for 28.3% of global breast cancer DALYs in 2023.2
Premenopausal vs. Postmenopausal Burden
Risk factor impacts varied by menopausal status:2,17
•Postmenopausal women had 33.6% of DALYs attributable to risk factors, with a high BMI contributing strongly.
•Premenopausal women showed a complex relationship with BMI, where an elevated BMI appeared to reduce risk marginally—consistent with established epidemiological patterns.
Increasing Cases and Deaths
By 2050, global breast cancer incidence is projected to reach:2
•3.56 million cases annually
•1.37 million deaths annually
These increases will occur even though ASIR and ASMR are expected to remain relatively stable. The primary drivers are population
growth, population aging, and increasing exposure to risk factors in transitioning countries.2,17
Regional Forecasts
Sub-Saharan Africa is expected to continue having the highest mortality burden, with ASMR projected to increase from 29.8 to 32.8 per 100,000 by 2050—far above the global average. Conversely, high-income regions are expected to maintain relatively low and stable mortality rates.2
Early Detection and Timely Diagnosis
The World Health Organization's Global Breast Cancer Initiative emphasises three pillars: education and awareness, timely diagnosis, and comprehensive treatment.18 Evidence from Rwanda, Pakistan, and Tajikistan illustrates that low-cost strategies—such as community education and clinical breast examination training—can meaningfully improve early detection rates.19,20
Expanding Treatment Capacity
Many low-resource regions lack essential components of breast cancer care:10,12,21
•radiotherapy machines
•pathology services
•specialised surgery
•hormone therapy and chemotherapy availability
To address these gaps, it is critical to expand capacity—investing in infrastructure, training healthcare professionals, and ensuring reliable access to medicines and technologies—so that comprehensive breast cancer treatment becomes feasible and sustainable in these settings.
Reducing Financial Toxicity
Cancer treatment costs can devastate households, particularly in LMICs. Expanding universal health coverage, increasing insurance coverage for cancer, and reducing the cost of essential medicines (e.g., through generic production and pooled procurement) are crucial steps. Targeted investment, technology transfer, procurement transparency, and international partnerships will be critical.22
Despite impressive global advancements, breast cancer continues to impose an expanding and unequal burden. High-income countries have achieved substantial reductions in mortality through robust screening programs, early diagnosis, and high-quality treatment. Meanwhile, low- and middle-income countries face rising incidence and worsening mortality, fuelled by demographic transition, limited access to timely care, and escalating risk factor exposure.
Forecasts to 2050 underscore that without decisive action, breast cancer will increasingly strain health systems and widen global health inequities. A comprehensive, equity-oriented strategy—bolstering early detection, strengthening treatment infrastructure, mitigating risk factors, and reducing financial barriers—is essential to safeguard global progress in women’s health and ensure that all women, regardless of geography or income, have the opportunity to survive and thrive after breast cancer.