An Uncomplicated, Yet Complex Target:'Single'Disease Perspectives of HZ Vaccination
HZ occurs when cell-mediated immunity falls due to ageing or immunosuppression, allowing latent varicella-zoster virus (VZV) infections to reactivate.8 Nearly all cases of HZ result in painful skin lesions, and if not treated immediately, it often can lead to post-herpetic neuralgia amongst other potential longer-term complications. Indeed, 95% of individuals over 50 years of age have had prior VZV exposure, and individuals who live to 85 years old have an approximately 50% lifetime risk of developing HZ.9
Currently, two vaccines against HZ exist: 1) the live, attenuated zoster vaccine, and 2) the non-live, recombinant zoster vaccine, with the latter showing higher and longer-lasting estimates of efficacy. Yet studies on cost-benefit analyses have varied
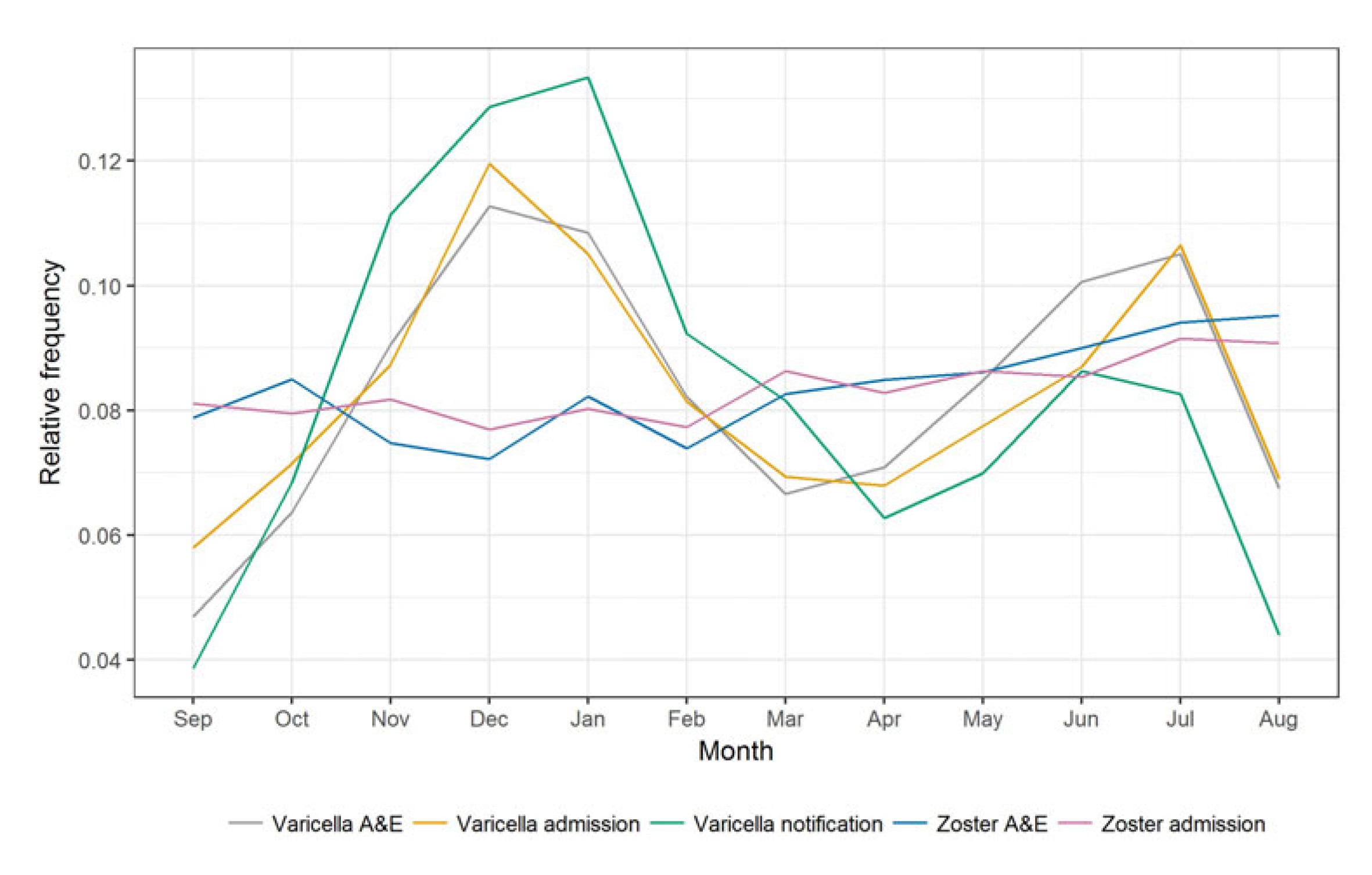
results, potentially since HZ has low mortality and incidence in later life (equating to lower economic productivity).10,11 Nevertheless, the rise in HZ likely owes much to ageing populations, increasing chronic disease, the use of immunosuppressive medications, as well as changes in health-seeking behaviour and more comprehensive disease surveillance.12 Lower VZV circulation from widespread varicella vaccination in childhood immunisation programmes also reduces the exogenous boosting, immunological mechanisms that encourage HZ immunity. That being said, evidence of increased HZ incidence predates mass varicella vaccination, including in Hong Kong (Figure 1).13
Expanding Vaccination Targets:'Multi-'Disease Perspectives of HZ Vaccination
An increasing body of work is recognising that the immunological/protective benefits of HZ vaccination, as well as other vaccines, exist beyond their intended target. This suggests the value of moving beyond the single disease perspective, to consider the broader, multi-disease and overall public health benefits of vaccines. HZ affects the nervous system, and studies in mouse and human tissue models have linked herpesviruses to the hallmarks of Alzheimer's disease: amyloid beta production, tau phosphorylation, and neuroinflammation, that arise as a protective response to acute infection, but becomes maladaptive during chronic infections.3,4,8
Other studies have compared individuals who chose to be vaccinated or not, to understand the potential link between HZ vaccination and dementia prevention, but are often limited by potential confounding factors such as diet, socioeconomics, physical activity and more.4 Meanwhile, on top of their previous natural experiments of HZ vaccination and dementia in Wales and Australia, Pomirchy et al. (2026) recently published their analysis on their natural experiment of live, attenuated HZ vaccination and dementia onset in Canada, to strengthen the evidence base on any causal links.4
Natural Experiment Methodology
Randomised controlled trials (RCTs) remain the gold standard of pharmaceutical interventions, but such design may not be ethical, feasible, or appropriate to investigate policy changes, programme introductions, or structural interventions common to public health initiatives. In particular, confounding factors that are 'controlled' for in RCTs become important contextual factors in the real-world. Natural experiments are more aligned to public health research — tracing back to John Snow’s work in understanding London's cholera epidemics in the mid-nineteenth century; they now sit in the realm of ‘evidence-based’ research, and are popular in other fields such as economics, education, agriculture, social work, engineering, and urban planning. Broadly speaking, natural experiments are on an event (or when ‘early adopters’ implement an intervention) that is not under the control of a researcher, that divide a population into exposed and unexposed groups.14
In their natural experiment study, Pomirchy et al. (2026) looked at the introduction of publicly funded HZ vaccination in adults aged between 65–70 years on September 15, 2016 in Ontario, Canada. They also offered HZ vaccination between September 15 to December 31, 2016 to people born in 1945 (71 years old that year). This naturally created three groups: 1) eligible (aged 65–70 years on Sept 15, 2016), 2) eligible for 3.5 months (aged 71 in 2016); and 3) ineligible (born before 1945). The primary analysis focused on comparing those eligible for at least 1 year and 3.5 months to those ineligible, assuming that other than HZ vaccination, individuals are similar/balanced in observed and unobserved characteristics. The outcome of new dementia diagnoses in the 5.5-year follow-up period was identified based on a pan-Canadian electronic health record database for primary care.4
Pomirchy et al. (2026) found that 4.3% of vaccine-eligible patients (n=8,795) and 5.3% of vaccine-ineligible patients (n=6,997) had a new dementia diagnosis during follow-up, with vaccine eligibility decreasing the probability of receiving a new dementia diagnosis by an absolute difference of 2.0 percentage points (95% CI 0.4–3.5, p=0.012). A regression discontinuity analysis and multiple hypothesis testing for the quasi-randomised design found no biases in the data. Similarly, when controlling for diagnoses of the 15 most common clinical conditions at baseline, vaccine eligibility still reduced new diagnoses of dementia over the 5.5-year follow-up by 1.9 percentage points (95% CI 0.4–3.4, p=0.016). Interestingly, the effect of vaccine on new diagnoses of dementia was significant among female but not among male individuals, shedding further light on the immunological differences between males and females.4
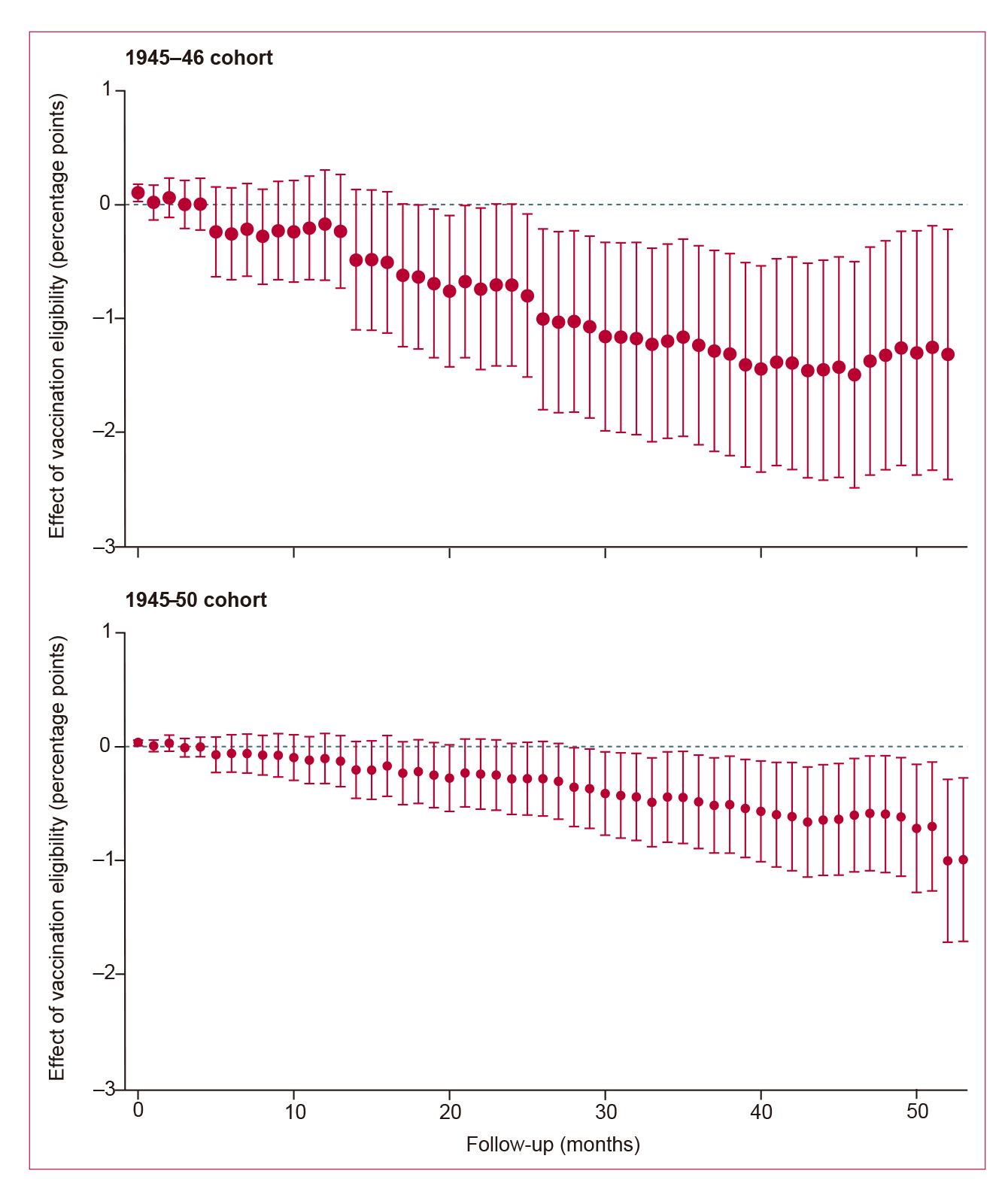
The authors also compared the vaccine-eligible cohort in Ontario to other provinces in Canada. Not only did they find near-identical trends in dementia incidence before the vaccination programme was introduced, but incidence of new dementia diagnoses was significantly lower among the vaccine-eligible birth cohort (born between Jan 1, 1945, and Dec 31, 1946) in Ontario than in the same birth cohort in other provinces after the vaccination programme (Figure 2). Similar results with the secondary analysis (comparing those eligible for only 3.5 months) support the causal effect.4
In a similar vein, the effects of HZ vaccination have been studied in biological ageing. A population-based cohort study of 3,884 adults >70 years with previous HZ vaccination in the US showed improvements in inflammation, innate and adaptive immunity, cardiovascular haemodynamics, neurodegeneration, epigenetic and transcriptomic ageing, as well as composite biological ageing score. The effects were most pronounced within the three-years after vaccination, but had unclear longitudinal effects.5
HZ infection and HZ vaccination with the live, attenuated virus have also been linked to cardiovascular health. A retrospective cohort study of 27,093 adults in the US with chronic disease demonstrated a lower risk of stroke (1.61% vs 2.20%; p<0.05) and myocardial infarction (1.29% vs 1.82%; p<0.05) in vaccinated versus unvaccinated individuals, even when controlling for comorbidities, although differences resulting from socioeconomic status could not be determined.6 Another longer-term, nationwide study in South Korea of 1,271,922 individuals aged ≥50 years showed reduced cardiovascular disease risk (HR=0.77, 95% CI 0.76–0.78). They also found that the greatest reduction was observed 2–3 years after vaccination, similar to the study on biological ageing, and persisted up to eight years.5,7 The Korean study also found that the cardiovascular benefits were greater in those from low-income households and rural residents. While the evidence is still unfolding, the effects of HZ vaccination beyond HZ morbidity are worth considering.7
A New Vaccine Paradigm: Public Health Perspectives of HZ Vaccination
An active area of discussion in the public health literature involves calling for a new vaccine paradigm: one that considers the wider effects vaccines have on the overall population, rather than the traditional approach of a single vaccine for each infectious target.3 Benns et al. (2020) cited the epidemiological research on childhood vaccines, as well as immunology studies on live vaccines specifically.3 For example, studies of the measles, mumps, and rubella vaccine from high-income settings demonstrated reductions in respiratory infections amongst others, and that in low-income countries, the reductions in all-cause mortality attributed to measles vaccination were much larger (>50%) than anticipated. Live vaccines also induced innate immune training, producing stronger proinflammatory responses to unrelated antigens; and RCTs comparing live and inactivated vaccines in Bangladesh and Finland found that the live oral polio vaccine was associated with lower risks of diarrhoea and otitis media than the inactivated polio vaccines.3
HZ vaccination’s role in public health can be understood with the analogy of the rotavirus vaccine, which has lower efficacy in low-income settings, likely owing to co-infecting pathogens and malnutrition.15 An RCT showed lower vaccine effectiveness in Malawi than in South Africa (49.4% vs. 72%), yet the number of prevented episodes of severe rotavirus gastroenteritis was greater in Malawi, suggesting that vaccines have extra public health value where healthcare services are more limited.16 For rotavirus, the interrelated burden of diarrhoea, stunting, and metabolic disease encourages a shift-in perspective to long-term disease prevention.15 Similarly, HZ’s links to pathological ageing and cardiovascular conditions may encourage recognising the role HZ vaccination may play against non-communicable conditions and in addressing health disparities—a public health priority of the past decade with a significance that cannot be understated.17
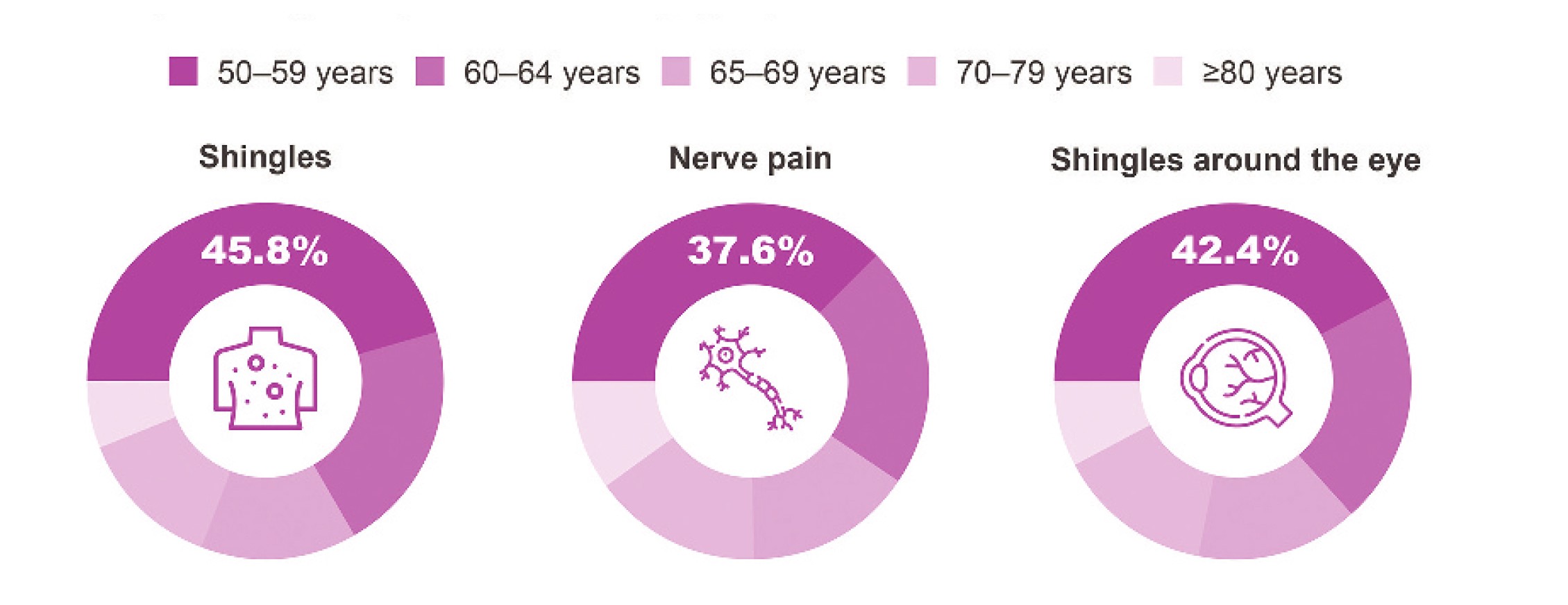
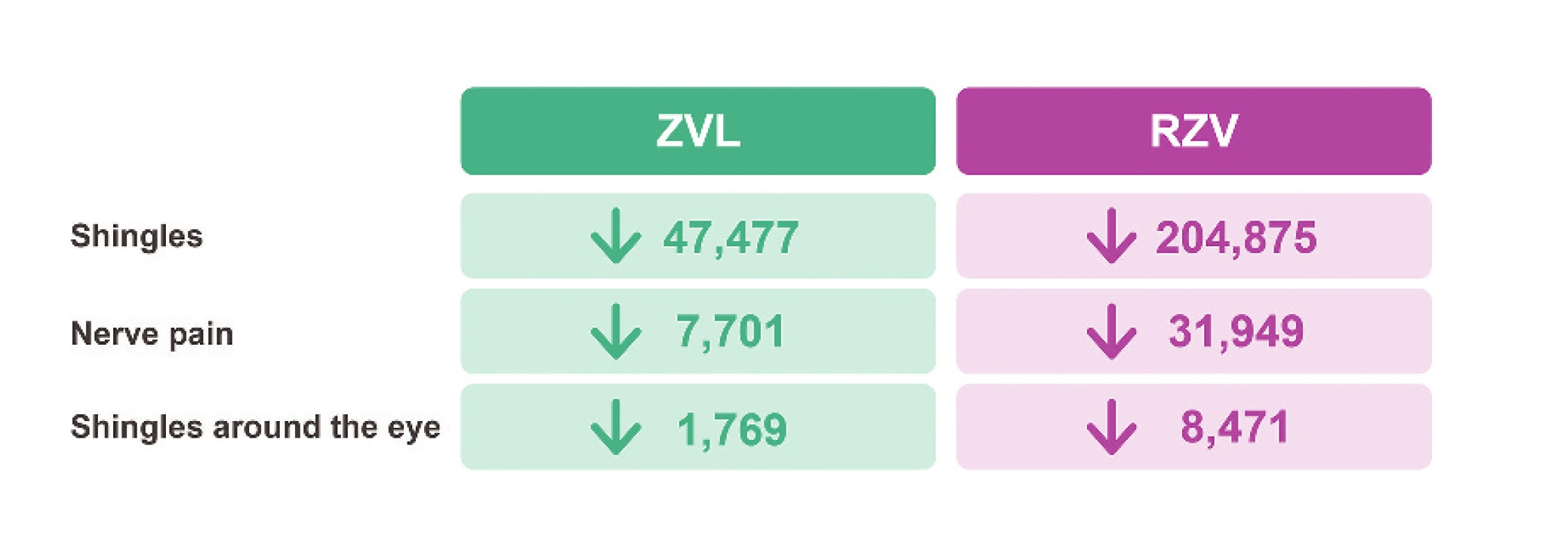
However, usage of the non-live, recombinant zoster vaccine is increasing in Hong Kong and other countries.8 A modelling study based in Hong Kong by Chan et al. (2023) found that mass vaccination with the non-live, recombinant zoster vaccine is expected to considerably reduce public health burden of HZ among individuals ≥50 years compared with no vaccination or the live vaccine, as well as in preventing complications
(Figure 3).8 It also supported earlier vaccinations from age 50 rather than later, with the most cases avoided between the ages of 50-59.8 Whether non-live HZ vaccines have similar off-target health effects remains to be seen.
Can Vaccination Influence Public Health?
A more holistic vaccine paradigm would affect how vaccines are evaluated and how vaccination policy decisions are made.3 Indeed, attempts have been made to revamp vaccine assessment strategies to capture their tangible and intangible value.1 It has also opened the realm of vaccinology development to innate immunity-training vaccines.3 Ultimately, vaccines must be effective for their primary target, but considering their multitude of health effects may lead the way on new public health strategies and potentially influence both societal attitudes and vaccine acceptance.
a)
b)