Cognitive reserve can be understood as the brain’s ability to “improvise”—to recruit alternative networks, cognitive strategies, or compensatory mechanisms to maintain performance when confronted with damage or increased demand. Rather than reflecting brain size or neuron count alone, cognitive reserve represents a functional adaptability developed over a lifetime of learning, curiosity, problem-solving, and engagement with the environment.1
Clinically, the importance of cognitive reserve lies in its ability to explain why individuals with similar degrees of neuropathology can experience markedly different cognitive outcomes. Two patients may show comparable amyloid plaques or vascular lesions on imaging or at autopsy, yet one remains functionally intact while the other develops overt dementia. Cognitive reserve provides a framework for understanding this variability and offers a target for preventive strategies.2
The concept of cognitive reserve emerged in the late 1980s, when neuropathologists reported a paradoxical finding: some individuals who had no documented cognitive impairment during life were found at autopsy to have extensive brain changes consistent with advanced Alzheimer’s disease. These included significant amyloid deposition, neurofibrillary tangles, and cortical atrophy.3
Early work by Katzman and later formalised by Stern and colleagues proposed that education, occupational complexity, and intellectual engagement allowed certain individuals to tolerate a greater burden of pathology before clinical symptoms emerged. Cognitive reserve, as distinct from “brain reserve” (a purely structural notion), emphasised flexible and efficient neural processing rather than passive protection. Since then, cognitive reserve has been supported by epidemiological, neuroimaging, and clinical studies, becoming a cornerstone concept in aging and dementia research.4,5
Cognitive reserve is not a single biological entity but a multifaceted process involving several overlapping mechanisms:6
• Neural Efficiency: Individuals with higher cognitive reserve often show more efficient use of neural networks, requiring less activation to perform the same cognitive tasks.
• Neural Compensation: When primary networks are compromised, alternate or secondary networks can be recruited to maintain function.
• Cognitive Strategy Flexibility: Higher reserve allows individuals to adopt different problem-solving strategies when familiar ones fail.
• Synaptic Plasticity: Lifelong learning enhances synaptic density and connectivity, supporting adaptability in the face of injury or degeneration.
Importantly, cognitive reserve is dynamic. It can be strengthened or eroded throughout life depending on health behaviours, environmental exposures, and psychosocial factors.5
Dementia and Alzheimer’s Disease
The strongest evidence for cognitive reserve comes from Alzheimer’s disease research. Numerous cohort studies demonstrate that higher educational attainment, intellectually demanding occupations, and active lifestyles are associated with delayed onset of clinical dementia—even when neuropathological burden is high.7
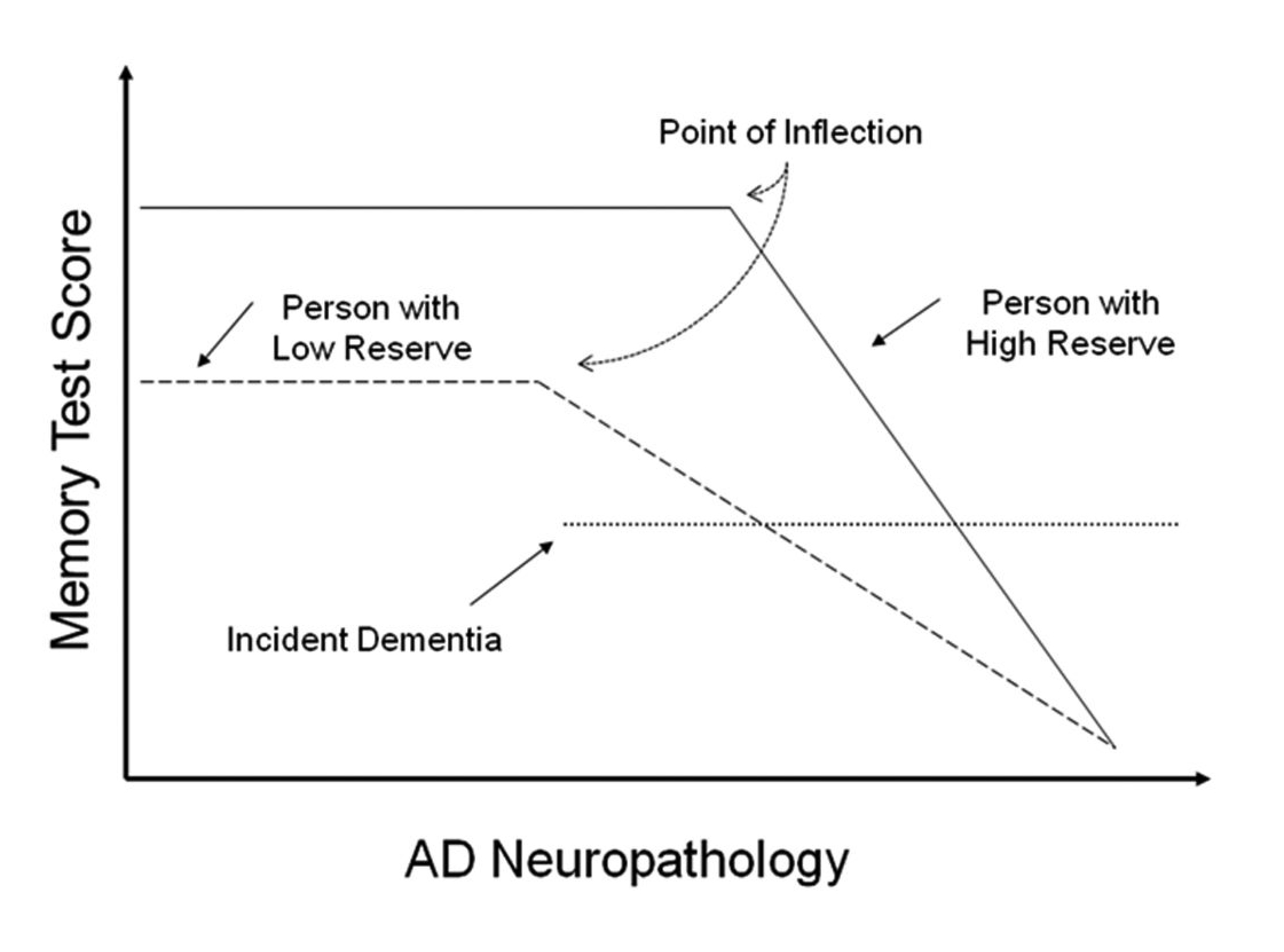
However, an important clinical nuance is that once symptoms do appear in individuals with high cognitive reserve, decline may be more rapid (Figure 1). This reflects the fact that pathology has already progressed substantially before clinical thresholds are crossed.8
Other Neurological Conditions
Cognitive reserve is not limited to Alzheimer’s disease. A robust reserve has been associated with:9
• Better functional outcomes after stroke
• Delayed cognitive impairment in Parkinson’s disease
• Improved coping and preserved function in multiple sclerosis
• Greater resilience following traumatic brain injury
In each case, cognitive reserve acts as a buffer, allowing patients to maintain independence for longer despite neurological insult.9
Beyond chronic neurodegeneration, cognitive reserve plays a critical role in responding to acute or subacute challenges. Major stressors—such as surgery, hospitalisation, toxin exposure, or prolonged psychological stress—place increased demands on cognitive systems. In these situations, the brain may need to “shift gears,” deploying additional cognitive resources to maintain normal function.10
Patients with higher cognitive reserve often show:10
• Lower risk of postoperative cognitive dysfunction
• Better stress tolerance and emotional regulation
• Enhanced recovery following illness or injury
For HCPs, this underscores the importance of assessing lifestyle and cognitive engagement when evaluating risk and resilience.1
While genetics contribute to cognitive reserve, lifestyle factors are the most modifiable and clinically actionable components. Researchers at Harvard Medical School have identified six interdependent cornerstones of brain health and cognitive fitness. Importantly, these elements work synergistically; no single intervention is sufficient in isolation:11
Step 1: Eat a Plant-Based Diet
A diet emphasising fruits, vegetables, whole grains, legumes, nuts, and healthy fats supports cognitive reserve through multiple mechanisms:
• Reduction of oxidative stress and inflammation
• Improved vascular health
• Enhanced gut–brain axis signalling
Mediterranean and MIND (Mediterranean-DASH diet Intervention for Neurodegenerative Delay) dietary patterns have been consistently associated with slower cognitive decline and reduced dementia risk. These diets support neuronal health while minimising metabolic and vascular insults that erode reserve over time.
Step 2: Exercise Regularly
Physical activity is one of the most powerful modulators of brain health. Aerobic and resistance exercise:
• Increase cerebral blood flow
• Promote neurogenesis in the hippocampus
• Upregulate brain-derived neurotrophic factor (BDNF)
• Improve executive function and memory
Regular exercise not only builds cognitive reserve but also amplifies the benefits of other lifestyle interventions, such as improved sleep and stress reduction.
Step 3: Get Enough Sleep
Sleep is essential for memory consolidation, synaptic homeostasis, and metabolic waste clearance via the glymphatic system. Chronic sleep deprivation is associated with increased amyloid accumulation and impaired attention, learning, and executive function.
For adults, consistent sleep duration and quality are critical for preserving cognitive reserve and preventing long-term cognitive vulnerability.
Step 4: Manage Stress
Chronic psychological stress negatively affects cognitive reserve through sustained cortisol exposure, hippocampal atrophy, and impaired neuroplasticity. Stress management techniques—including mindfulness, relaxation training, and cognitive behavioural strategies—help protect neural integrity.
Clinicians should recognise stress not only as a mental health issue but as a modifiable risk factor for cognitive decline.
Step 5: Nurture Social Contact
Social engagement stimulates cognitive, emotional, and language networks simultaneously. Strong social ties are associated with reduced dementia risk and better cognitive performance in aging populations.
Isolation and loneliness, in contrast, are linked to accelerated cognitive decline, depression, and increased mortality. Encouraging social interaction is therefore a critical, yet often overlooked, component of cognitive reserve building.
Step 6: Continue to Challenge the Brain
Lifelong learning remains central to cognitive reserve. Activities that challenge the brain—such as learning new skills, engaging in complex tasks, reading, or problem-solving—promote neural flexibility.
Importantly, novelty and difficulty matter. Passive activities that do not require active engagement confer fewer benefits than those that demand sustained attention and adaptation.
These six cornerstones form a cohesive plan rather than a checklist of independent actions. Improving diet without addressing sleep, or exercising without managing stress, yields limited benefit. Cognitive reserve is built through cumulative, interacting behaviours that collectively enhance brain resilience.11
For HCPs, this integrated framework supports a shift from reactive disease management to proactive cognitive health promotion.
Cognitive reserve provides a unifying concept for understanding resilience in brain aging, neurological disease, and life stress. Rooted in decades of clinical observation and research, it explains why some individuals maintain cognitive function despite significant pathology and why lifestyle interventions can meaningfully alter cognitive trajectories.
For HCPs, cognitive reserve highlights the importance of early, sustained lifestyle counselling as a core component of preventive care. By promoting plant-based nutrition, regular physical activity, adequate sleep, stress management, social engagement, and lifelong learning, clinicians can help patients build and preserve cognitive reserve—supporting functional independence and quality of life well into older age.